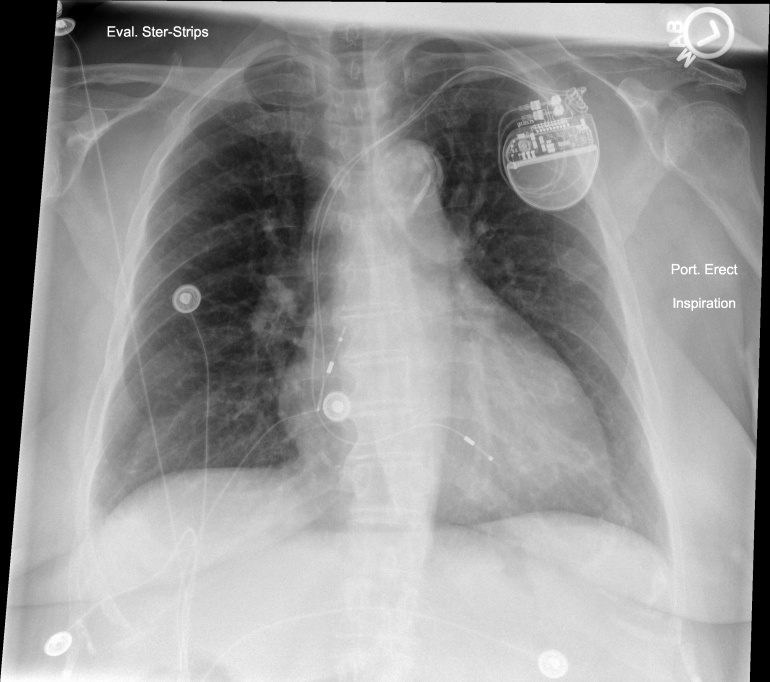
The following PA and Lateral CXR was obtained the day after an uneventful dual chamber pacemaker implantation placed via left cephalic cutdown.
One can see a radiopaque ribbon near the pacemaker can in both views raising the suspicion of a retained operative sponge. All skin dressings were removed and repeat CXR was performed.
Repeat PA CXR performed after dressing removed leaving steri-strips in place reveals that wound dressing had inadvertently used a radiopaque lap sponge as part of a pressure dressing. Nice case of “pseudo” sponge in the pocket but certainly caused some initial stress during CXR reading!
This is the fifth in a series of short (less than 5minutes), educational videos designed for patients and their care providers to develop a thorough understanding of pacemakers. Lecture 5 What to Expect on the Day of Pacemaker Implant Procedure describes the events that take place on the day of pacemaker implantation. Important topics include hospital registration and check-in, the implant procedure, and post-implant events.
Please see the Patient Education section of Heart Rhythm Center for other lectures in this series.
This is the fourth in a series of short (less than 5minutes), educational videos designed for patients and their care providers to develop a thorough understanding of pacemakers. Lecture 4 Preoperative Workup and Evaluation (Meeting the Implanting Physician) describes the preoperative evaluation for patients preparing to undergo pacemaker implantation. Important topics include the types of physicians that perform pacemaker implantation and questions to ask the doctor to minimize the risk of complications.
Please see the Patient Education section of Heart Rhythm Center for other lectures in this series.
This is the third in a series of short (less than 5minutes), educational videos designed for patients and their care providers to develop a thorough understanding of pacemakers. Lecture 3 What are Pacemakers and How Do They Work? describes the basics of pacemaker implantation and how the pacemakers work.
Your care providers have extensive training assessing the reasons—also called indications—that a patient may need a pacemaker. In particular, it is very important that the benefits of pacemaker implantation outweigh the risks of the pacemaker implant surgery (to be discussed later). The American College of Cardiology (ACC) is one of the major professional societies that develops guidelines to help care providers make educated clinical decisions that are based upon prior clinical studies. This is the basis of “evidence-based” medicine: the process by which clinical ideas are tested, reported, and reevaluated to decide the most appropriate care for a particular condition.
The ACC has developed guidelines that help care providers decide when a patient would be best served by a pacemaker. The easiest rule to remember is: pacemakers are most appropriate for patients who are having symptoms related to an abnormally slow—or at times, fast—heart rate. These symptoms include: shortness of breath, chest pain, dizziness, fainting (also called syncope), heart failure, arrhythmias (such as ventricular tachycardia/fibrillation), or fatigue. The decision to implant a pacemaker also requires evaluation of the permanence of the AV block. Electrolyte abnormalities (like potassium) can cause significant AV block, but correction of the abnormality can lead to resolution of the AV block. Some diseases—like Lyme Disease—often follow a natural course where the AV block is temporary and resolves as the disease is treated. Some types of AV block that occur during periods of vagal activation can reverse very quickly (e.g., nausea and dizziness during a blood draw may cause transient AV block or during sleep in patients with sleep apnea). In addition, after aortic valve surgery, inflammation can cause transient AV block that resolves within days of the operation. Finally, there are some diseases that warrant pacemaker implantation, because the AV block may continue to worsen (for example, sarcoidosis, amyloidosis, or neuromuscular diseases).
This is the second in a series of short (less than 5minutes), educational videos designed for patients and their care providers to develop a thorough understanding of pacemakers. Lecture 2 Reasons for Pacemaker Implantation describes some of the common reasons patients undergo pacemaker implantation.
Your care providers have extensive training assessing the reasons—also called indications—that a patient may need a pacemaker. In particular, it is very important that the benefits of pacemaker implantation outweigh the risks of the pacemaker implant surgery (to be discussed later). The American College of Cardiology (ACC) is one of the major professional societies that develops guidelines to help care providers make educated clinical decisions that are based upon prior clinical studies. This is the basis of “evidence-based” medicine: the process by which clinical ideas are tested, reported, and reevaluated to decide the most appropriate care for a particular condition.
The ACC has developed guidelines that help care providers decide when a patient would be best served by a pacemaker. The easiest rule to remember is: pacemakers are most appropriate for patients who are having symptoms related to an abnormally slow—or at times, fast—heart rate. These symptoms include: shortness of breath, chest pain, dizziness, fainting (also called syncope), heart failure, arrhythmias (such as ventricular tachycardia/fibrillation), or fatigue. The decision to implant a pacemaker also requires evaluation of the permanence of the AV block. Electrolyte abnormalities (like potassium) can cause significant AV block, but correction of the abnormality can lead to resolution of the AV block. Some diseases—like Lyme Disease—often follow a natural course where the AV block is temporary and resolves as the disease is treated. Some types of AV block that occur during periods of vagal activation can reverse very quickly (e.g., nausea and dizziness during a blood draw may cause transient AV block or during sleep in patients with sleep apnea). In addition, after aortic valve surgery, inflammation can cause transient AV block that resolves within days of the operation. Finally, there are some diseases that warrant pacemaker implantation, because the AV block may continue to worsen (for example, sarcoidosis, amyloidosis, or neuromuscular diseases).
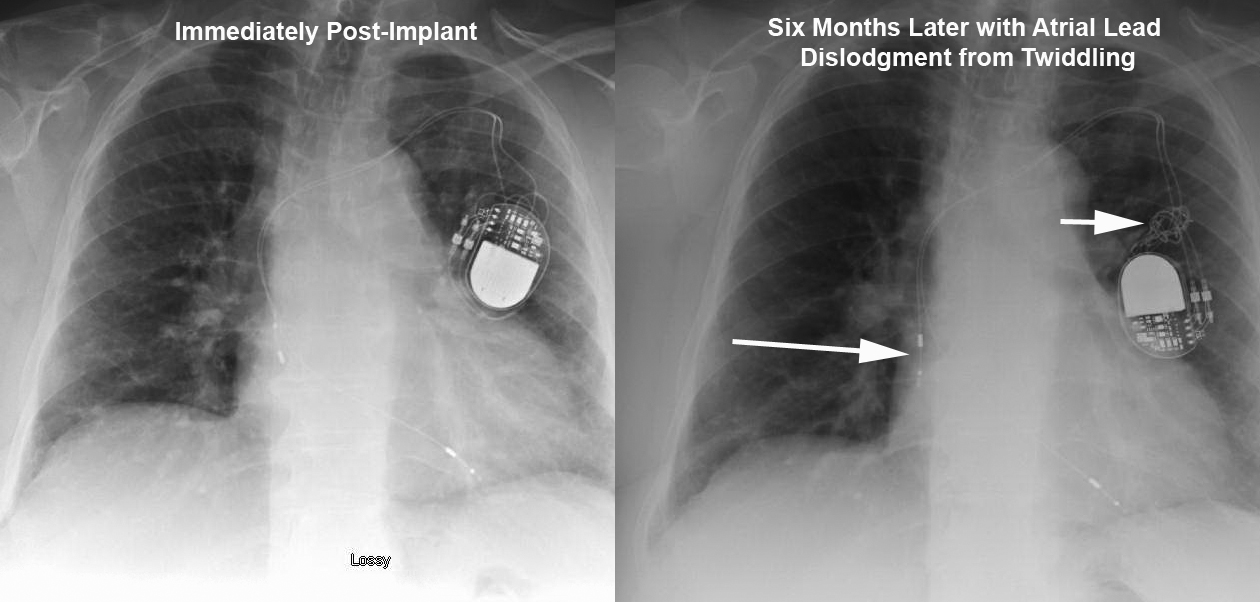
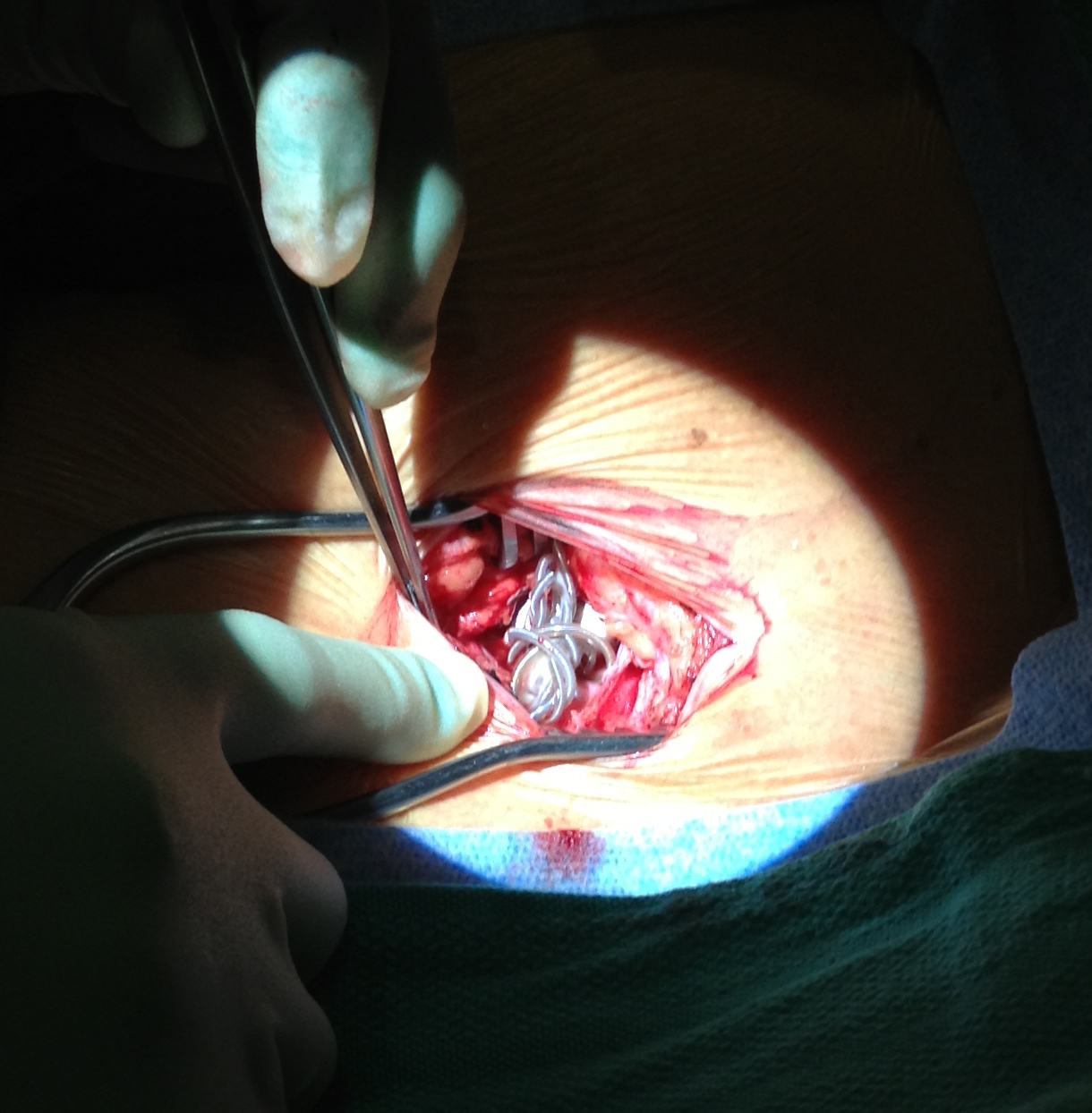
This elderly patient presented 6months after a dual chamber pacemaker was implanted due to symptomatic chronotropic incompetence. They reported recurrence of exertional shortness of breath that was experienced before pacemaker implantation. Device interrogation revealed complete loss of capture in the atrial lead. The top Figure depicts lead orientation before (left) and after (right) patient twiddling resulted in loss of slack in both leads with frank atrial lead dislodgement. Arrows show the dislodged atrial lead and knotted leads. The bottom Figure shows the intraoperative finding of knotted leads in the pocket. The leads were carefully unknotted, stylets placed, and leads repositioned with normal parameters. Originally described in 1968 [1], twiddling refers to patient manipulation of pacemaker can or leads that may lead to malfunction. It has a reported incidence of 0.07% in a series of 17000 patients. [2] The patient underwent an uneventful lead revision by repositioning the atrial lead and adding slack to the ventricular lead.
1 Bayliss CE, Beanlands DS, Baird RJ, “The pacemaker-twiddler’s syndrome: a new complication of implantable transvenous pacemakers,” Can Med Assoc J, V. 99 (1968), pp. 371–3.
2 T. Fahraeus and C. J. Hoijer, “Early pacemaker twiddler syndrome,” Europace, Vol. 5 (July 2003), pp. 279-281.
This is the first in a series of short (less than 5minutes), educational videos designed for patients and their care providers to develop a thorough understanding of pacemakers. Lecture 1 The Basics of Heart Anatomy and Conduction System introduces the core concepts of heart function necessary to understand the role of pacemakers in the management of heart disease.
Please check back for future lectures to be posted and register to receive updates from the Heart Rhythm Center.
Lecture 2: Reasons for Pacemaker Implantation
Lecture 3: What are Pacemakers and How Do They Work?
Lecture 4: Preoperative Workup and Evaluation
Lecture 5: Meeting the Implanting Physician
Lecture 6: The Implant Procedure
Lecture 7: Possible Complications of Pacemaker Implantation
Lecture 8: Post-operative Care of the Pacemaker Patient (The First Month)
Lecture 9: Long-Term Care and Follow-up of the Pacemaker Patient
Lecture 10: What are Pacemaker Device Recalls/Advisories/Alerts?
The fastest growing population segment in the United States, seniors commonly undergo pacemaker implantation. Although doctors’ offices typically provide short pamphlets on pacemaker implantation, there is rarely any comprehensive yet understandable reference material for the patients to obtain…until now. Explaining the “what, why, and how” of pacemaker implantation, this invaluable new guide provides an in-depth summary of pacemakers, from the initial patient evaluation and device implantation to the issues that could potentially arise during a long-term follow up.
A very active octogenarian with history of ischemic cardiomyopathy, CAD status post bypass surgery and congestive heart failure (CHF) presented for evaluation. He had a dual chamber defibrillator (ICD) implanted in 2006 because of sustained ventricular tachycardia (VT). His ejection fraction was 10-15% with extensive infarct and no evidence of ischemia on stress test. He was having shortness of breath with mild exertion (and resting at times) giving him Class 3/4 CHF. His electrocardiogram showed left bundle branch block and QRS duration of 160msec.
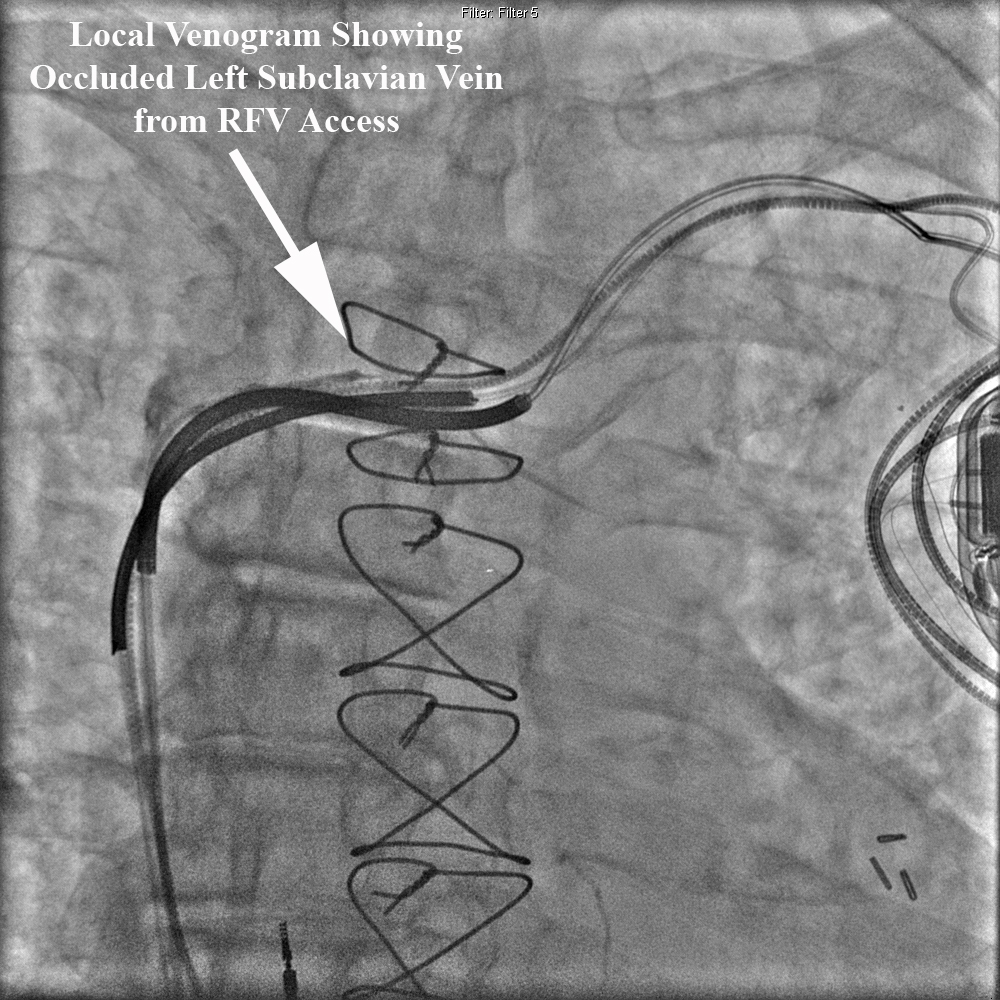
He was scheduled for upgrade of his defibrillator to a biventricular defibrillator with the addition of a left ventricular (LV) lead placed percutaneously in his coronary sinus. Of note, his initial right ventricular ICD lead (Medtronic Sprint Fidelis) had to be replaced several years ago. His in-situ ICD still had battery life and the decision was made to assess coronary sinus and left subclavian patiency prior to opening the ICD incision and risking device infection. Peripheral venogram of his left upper extremity revealed an occluded left subclavian vein in the midline (see Figure).
Right femoral venous access was obtained and a 5French deflectable octapolar EP catheter was used to document coronary sinus patency. At this point, access to the left subclavian vein was attempted with the EP catheter without success. A local venogram was then performed using a 5French multipurpose catheter and once again demonstrated an occluded left subclavian vein from the contralateral approach. See Figure below.
Given the patient’s extreme age, the decision was made not to attempt opening his chronic left subclavian venous occlusion or attempt laser lead extraction of the abandoned RV lead. We opted to place a coronary sinus LV lead via a patent right subclavian vein and percutaneously tunnel the lead to his existing left sided device. A 2cm incision was made in the right infraclavicular region and LV lead was placed without difficulty in a posterolateral branch of the coronary sinus. This lead was anchored to the right prepectoral fascia then tunneled subcutaneously to the exisiting left infraclavicular lead system. Tunneling was performed without incident and the patient underwent a successful upgrade to a biventricular defibrillator. The figure below depicts the chest xray and course of the tunneled LV lead. There was minimal postoperative discomfort along the course of the tunneled lead.
A study revealed at this year’s Heart Rhythm Society Meeting presented the first in-human results of a leadless implantable pacemaker. The device is about the size of a AAA battery and is implanted in the right ventricle. A limitation of current pacemakers is the reliance on implantable leads that can fracture or become infected. This device is the first step toward developing leadless pacing technologies. It remains to be seen how clinically useful this device will be but is expected to be available in Europe later this year.