Jeffrey Williams, MD, MS, FACC, FHRS, CPE and Gabriella Williams
James A Haley VA Medical Center and University of Notre Dame
Problem Statement or Scientific Question: There is consensus that the subcutaneous (SC) implantable cardioverter defibrillator (ICD) is associated with fewer lead-related complications albeit limited battery longevity (based on Ah) compared to transvenous (TV) ICD. The type of device implanted is a shared decision made by the implanting physician and patient however, the long term costs of the SC versus TV ICD when balancing complications and battery longevity are unclear.
Background/Project Intent: To model the cost and complication rate variations between the 0.8Ah SC ICD and 1.0Ah, 1.9Ah, and 2.0Ah battery single chamber TV ICD generator replacements in a model over 26 years.
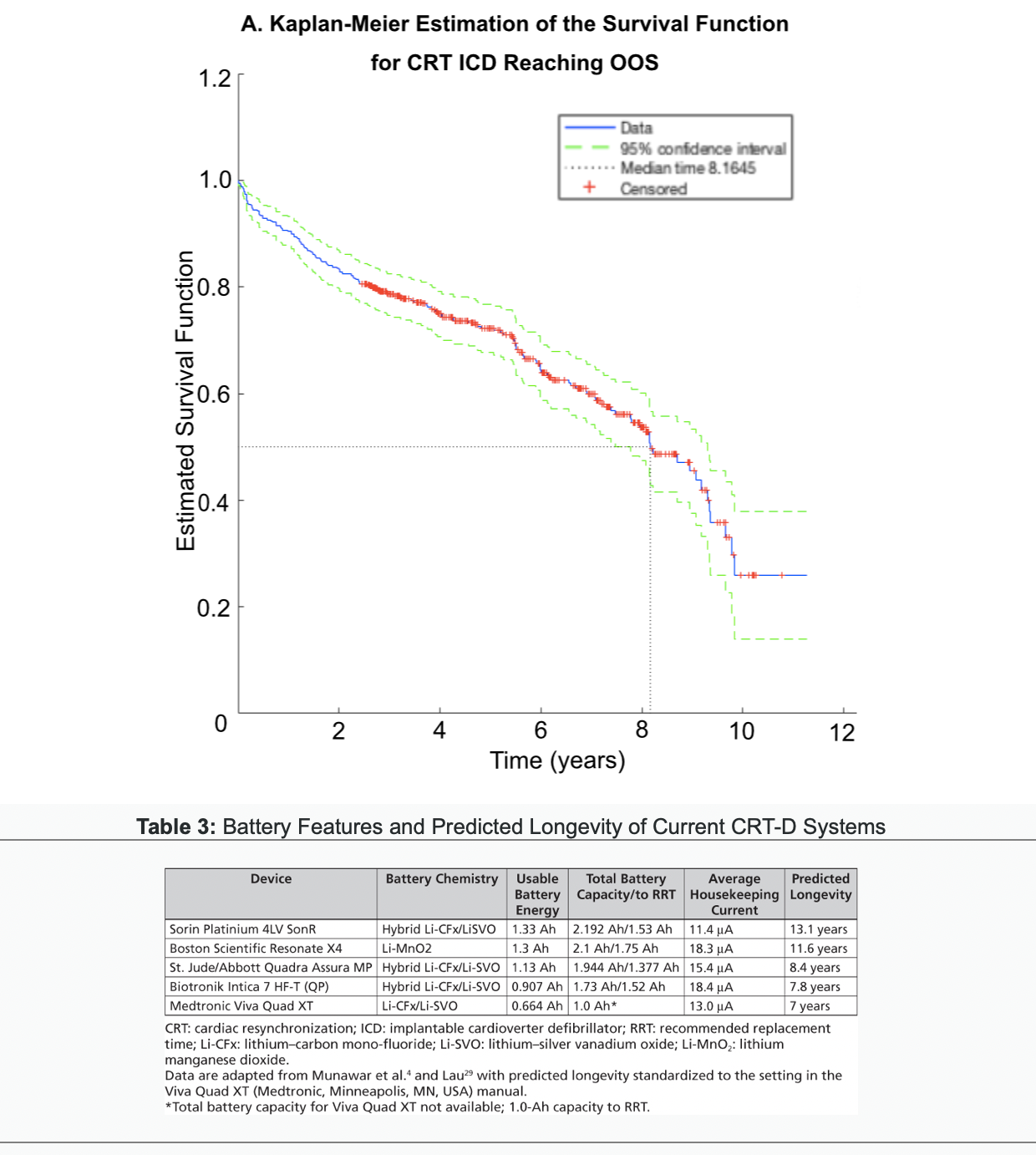
Methodology: A model was developed using MATLAB (Mathworks Inc., Natick, MA) estimating the rate of generator replacements of the SC ICD versus the TV-ICD (using 20% utilization for each device) to assess differences in costs and complications over time. Battery longevities were based upon prior “real-world” studies of CRT-D and extrapolated to single chamber TV ICD based upon current literature. Costs and baseline volumes for primary prevention ICD in the United States were based upon publicly available estimates. Model parameters including heart failure prevalence, mortality, and complication rates were based upon prior data.
Results: The 2.0Ah TV ICD had fewer generator replacements (max n=7200 annually) and costs (max annual savings of $247,500,000) compared to the SC ICD, 1.0Ah, and 1.9Ah TV ICD. The SC ICD had less generator replacement costs compared to the 1.0Ah and 1.9Ah TV ICD. The SC ICD was associated with fewer annual complications (max n=422) compared to all TV ICD.
Value Proposition: The 2.0Ah TV ICD reduced the total number of implant procedures for the patient. The 2.0Ah TV ICD was associated with lower costs for payers and society. The SC ICD had the fewest long-term complications.
Conclusions: The 2.0Ah TV ICD is associated with fewer replacement procedures and costs than smaller battery capacity TV ICD as well as SC ICD. The SC ICD had the fewest long-term complications when compared to the TV ICD (all battery capacities). The decision on device implant type requires a complex informed consent discussion with the patient to address costs, number of replacement procedures, and overall long-term complication rates.
References:
Alam MB, Munir MB, Rattan R, Adelstein E, Jain S, Saba S. Battery longevity from cardiac resynchronization therapy defibrillators: differences between manufacturers and discrepancies with published product performance reports. Europace. 2017;19(3):421–424.
Williams JL and Williams GM, “Modeling long-term effect of biventricular defibrillator battery capacity on major complications and costs associated with replacement procedures.” Heart Rhythm Journal, V. 18, Issue 8, August 01, 2021: S396-S397.
Poli S, Boriani G, Zecchin M, FacchinD, Gasparini M, Landolina M, Pietro Ricci R, Lanera C, Gregori D, and Proclemer A, “Favorable Trend of Implantable Cardioverter-Defibrillator Service Life in a Large Single-Nation Population: Insights From 10-Year Analysis of the Italien Implantable Cardioverter-Defibrillator Registry. J Am Heart Assoc. 2019;8:e012759.
Cutler D et al, “Physician Beliefs and Patient Preferences: A New Look at Regional Variation in Health Care Spending,” Amer Econ Jour: Econ Policy, Vol 11, No 1, Feb 2019, pp. 192-221.
Caverly TJ et al, “Patient Preference in the Decision to Place Implantable Cardioverter-Defibrillators,” Arch Intern Med. 2012;172(14):1104-1107.