Saving money and improving quality should be a priority no matter how “small” the impact. By 2028, Medicare Trustees project Medicare does not meet either the Trustees’ short-range test of financial adequacy or long-range test of close actuarial balance.

Yiyan Liu and I presented our research today at ACC 2023 Annual Sessions.
Background: Prior modeling has demonstrated the extended battery longevity of biventricular defibrillator (CRT-D) reduced additional implant or replacement procedures, yet real-world evidence on health economics data is limited. This study reports the total direct medical costs to Medicare associated with CRT-D procedures.
Methods: A retrospective study was conducted using the 5% Medicare Standard Analytical Files (SAF). Patients with CRT-D implant or replacement between 1/2009 and 12/2020 in hospital settings were identified using ICD-9-PCS (00.54) and ICD-10-PCS (0JH609Z, 0JH639Z, 0JH809Z, 0JH839Z) codes supplemented with Current Procedural Terminology* (CPT®) codes (33225, 33249, 33263, 33264). Total direct medical costs to Medicare included costs for all claim types. To capture medical costs leading to and following the procedure, the costs were calculated for three time periods: a 30-day interval before the procedure, the procedure encounter period, and a 30-day interval after the procedure. All analyses were performed using the Instant Health Data (IHD) software (Panalgo, Boston MA, USA) and R, version 3.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
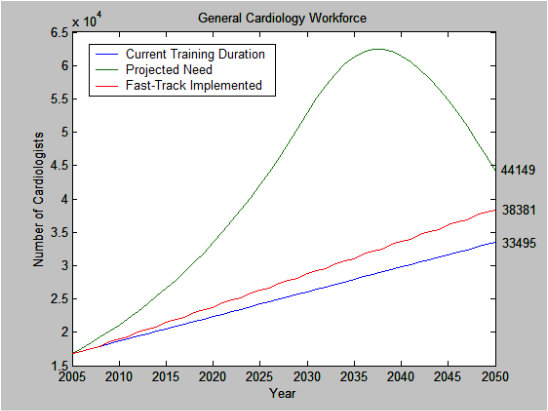
Results: Among the 15,002 Medicare patients who underwent CRT-D implant or replacement from 2009 through 2020, the mean age at first procedure was 72 and 71% were male. The number of patients with 1, 2, and 3 CRT-D procedures was 12,944, 1,923, and 135, respectively. The total cumulative cost to Medicare for an average patient undergoing 1, 2, and 3 generator implant or replacement procedures was $52,795, $88,976, and $128,846 in 2021 dollars, respectively (Figure).
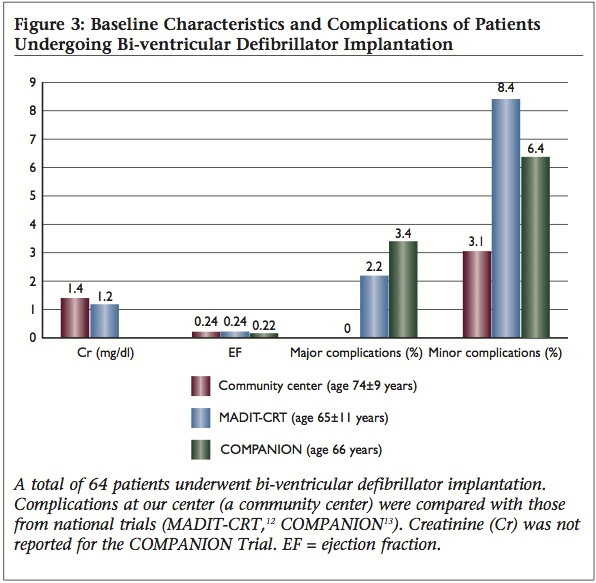
Discussion: Battery capacity as measured in ampere-hours (Ah) is the strongest predictor of CRT-D battery longevity. Extended defibrillator battery longevity is preferred by patients and cost savings for health care budgets. Data have demonstrated extended CRT-D extended battery life exceeded patient survival in a typical HFrEF cohort.1 These extended longevity CRT-D devices not only outlast patient life expectancy but avoid costs of complications and generator changes. The data presented here demonstrate the potential for a significant cost savings when fewer generator changes are required in Medicare patients due to battery depletion and when clinically appropriate.
CRT-D replacement due to battery depletion is a significant cost-driver for payors2,3 and a significant complication-driver for patients.4,5 Landolina et al. found the need for device replacements at six years was reduced from 83% to 68% with the use of devices with improved battery longevity from the most recent generation.2 Modeling has shown increased utilization of extended longevity CRT-D led to a 39% annual reduction in major complications (n=1099) and a 12.8% reduction in total annual costs ($496million) for Medicare.6 The data presented here indicate a 244% increase in cost when three CRT-D generator implant/replacement procedures were completed versus one were performed among 15,002 Medicare patients who underwent CRT-D implant or replacement from 2009 through 2020.
Limitations: This research used the number of generator implants/replacements as a surrogate for using extended battery longevity CRT-D; certainly, there will be incidences of device infection rather than battery depletion as indication for generator replacement. Prior data has shown the battery depletion is the most common cause of generator replacement even when using extended longevity CRT-D.6 These costs do not account for the nonfinancial or clinical outcome of additional complications resulting from more frequent generator changes. Finally, it is difficult to quantify the underlying systemic conflicts of interest where frequent CRT-D generator changes continue to drive fee-for-service or productivity-based reimbursements for physicians and health systems.
Conclusion: The total direct medical costs to Medicare for CRT-D implant or replacement increased substantially with increased procedure frequency.
References:
- Williams JL, Harley B, Williams G, “First Demonstration of Cardiac Resynchronization Therapy Defibrillator Service Life Exceeding Patient Survival in a Heart Failure with Reduced Ejection Fraction Cohort,” J Innov Cardiac Rhythm Manage. 2020; 11(12): 4325–4332.
- Landolina M, Morani G, Curnis A, et al. The economic impact of battery longevity in implantable cardioverter-defibrillators for cardiac resynchronization therapy: the hospital and healthcare system perspectives. Europace. 2017;19(8):1349–1356.
- Gadler F, Ding Y, Verin N, et al. Economic impact of longer battery life of cardiac resynchronization therapy defibrillators in Sweden. Clinicoecon Outcomes Res. 2016;8:657–666.
- Poole JE, Gleva MJ, Mela T, et al. Complication rates associated with pacemaker or implantable cardioverter-defibrillator generator replacements and upgrade procedures results from the REPLACE registry. Circulation. 2010;122(16):1553–1561.
- Prutkin JM, Reynolds MR, Bao H, et al. Rates of and factors associated with infection in 200,909 medicare implantable cardioverter-defibrillator implants: results from the NCDR®. Circulation. 2014;130(13):1037–1043.
- Williams JL and Williams GM, “Modeling long-term effect of biventricular defibrillator battery capacity on major complications and costs associated with replacement procedures.” Heart Rhythm Journal, V. 18, Issue 8, August 01, 2021: S396-S397.