A very active octogenarian with history of ischemic cardiomyopathy, CAD status post bypass surgery and congestive heart failure (CHF) presented for evaluation. He had a dual chamber defibrillator (ICD) implanted in 2006 because of sustained ventricular tachycardia (VT). His ejection fraction was 10-15% with extensive infarct and no evidence of ischemia on stress test. He was having shortness of breath with mild exertion (and resting at times) giving him Class 3/4 CHF. His electrocardiogram showed left bundle branch block and QRS duration of 160msec.
He was scheduled for upgrade of his defibrillator to a biventricular defibrillator with the addition of a left ventricular (LV) lead placed percutaneously in his coronary sinus. Of note, his initial right ventricular ICD lead (Medtronic Sprint Fidelis) had to be replaced several years ago. His in-situ ICD still had battery life and the decision was made to assess coronary sinus and left subclavian patiency prior to opening the ICD incision and risking device infection. Peripheral venogram of his left upper extremity revealed an occluded left subclavian vein in the midline (see Figure).

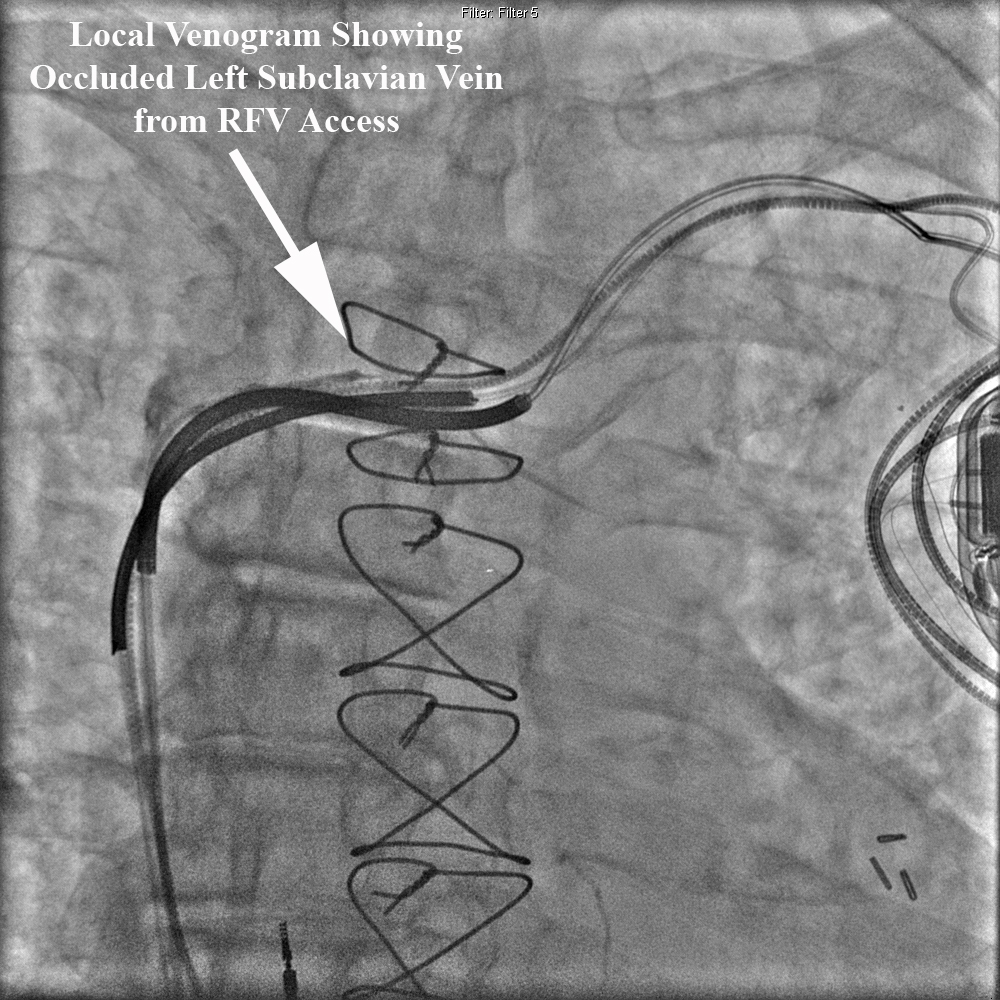
Right femoral venous access was obtained and a 5French deflectable octapolar EP catheter was used to document coronary sinus patency. At this point, access to the left subclavian vein was attempted with the EP catheter without success. A local venogram was then performed using a 5French multipurpose catheter and once again demonstrated an occluded left subclavian vein from the contralateral approach. See Figure below.
Given the patient’s extreme age, the decision was made not to attempt opening his chronic left subclavian venous occlusion or attempt laser lead extraction of the abandoned RV lead. We opted to place a coronary sinus LV lead via a patent right subclavian vein and percutaneously tunnel the lead to his existing left sided device. A 2cm incision was made in the right infraclavicular region and LV lead was placed without difficulty in a posterolateral branch of the coronary sinus. This lead was anchored to the right prepectoral fascia then tunneled subcutaneously to the exisiting left infraclavicular lead system. Tunneling was performed without incident and the patient underwent a successful upgrade to a biventricular defibrillator. The figure below depicts the chest xray and course of the tunneled LV lead. There was minimal postoperative discomfort along the course of the tunneled lead.

