A recent article from The Advisory Board Company found a group of hospitals that had an advantage when it came to providing an excellent patient experience: specialty hospitals. An Advisory Board analysis of recent Hospital Compare data suggests that specialty hospitals dominate the rankings when it comes to patient satisfaction.
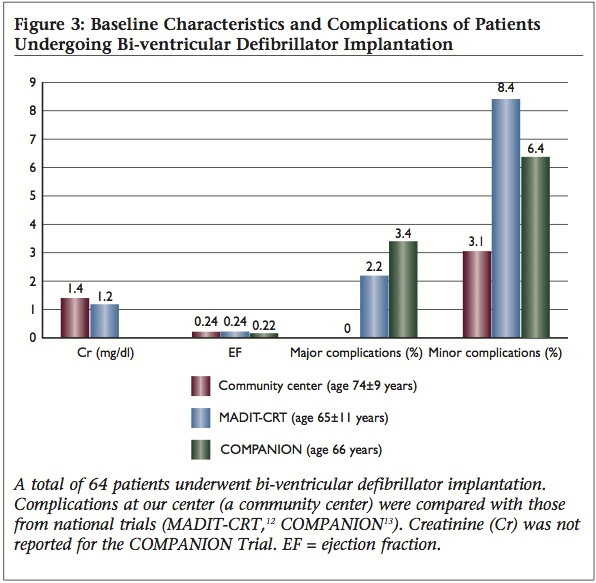
Patient satisfaction may not be the only benefit of a specialty hospital or “center of excellence.” We examined the demographics, complications, re-admissions, and accessibility of care in a community electrophysiology (EP) program to add to the body of knowledge of ‘real-world’ EP device implant complications. Two hundred and fifty consecutive patients who underwent device implantation by a single electrophysiologist in a new non-academic community hospital EP program starting from its inception in July 2008 were included for analysis. Standard procedures for implantation were used. Pacemakers, defibrillators, and generator changes were included; temporary pacemakers were excluded. Major complications were defined as in-hospital death, cardiac arrest, cardiac perforation, cardiac valve injury, coronary venous dissection, hemothorax, pneumothorax, transient ischemic attack, stroke, myocardial infarction, pericardial tamponade, and arteriovenous fistula. Minor complications were defined as drug reaction, conduction block, hematoma or lead dislodgement requiring re-operation, peripheral embolus, phlebitis, peripheral nerve injury, and device-related infection. This community cohort had similar ejection fractions but was older with worse kidney function than those studied in prior reports. There was one major early complication (0.4%) and seven minor early complications (2.8%). Left ventricular lead placement was successful in 64 of 66 patients (97%). This was the first community-hospital based EP program to examine device implant demographics and outcomes, and revealed an elderly, ill population with lower overall rates of complications than seen in national trials and available reports from single non-community centers. Contrary to current perceptions, these data suggest that community centers may subselect an elderly, ill patient population and can provide high-quality, cost-effective, and more accessible care.
“Specialty hospitals are under increasing scrutiny, but there may be a role for ‘niche’ hospitals that, while offering the full spectrum of general hospital care, can provide certain procedures at an exceptional level of quality and cost-effectiveness. Recent literature continues to document the paucity of data available on rates and predictors of ICD implantation in routine clinical practice.(24,25) The Ontario ICD Database (24) revealed major complications related to de novo defibrillator implantations in 4.1% of procedures. Adjusting our data to match their definition of major complications, our center had major complications in 1.0% of de novo defibrillator implantations (a 76% relative reduction in major complications). The cost of major complications among Medicare beneficiaries receiving implantable defibrillators was examined in 30,984 patients.(25) They found that 10.8% of patients experienced one or more complications resulting in an increase in length of stay by 3.4 days and costs by $7,251. Superiorly performing ‘niche’ hospitals that reduce major complication rates from defibrillator implants by 76% in the uS (conservative estimate of 100,000 yearly implants) could realize an estimated $60 million in cost savings while improving patient safety.” (Williams et al, 2010, full link to reference below)
Please take this one question poll about specialty hospitals:
For More Details Please See:
