This is the eleventh podcast in the What are Palpitations? series and we will be discussing the postoperative care following EP studies. We will cover care of the vascular access sites including showering/bathing restrictions. Other activity limitations including driving issues will be addressed. Finally, the first followup appointment after the EP study will be explained as well as lifestyle limitations that may be recommended.
Please check back with the Heart Rhythm Center for the final podcast in the What are Palpitations? series: Psychosocial Impact of Arrhythmias.
This is the tenth podcast in the What are Palpitations? series and we will be discussing the complications that can occur during or after EP studies. We begin the discussion with an explanation of the types of complications and their treatment. We will end by discussing special EP studies and ablations that may have higher rates of complications and lower success rates.
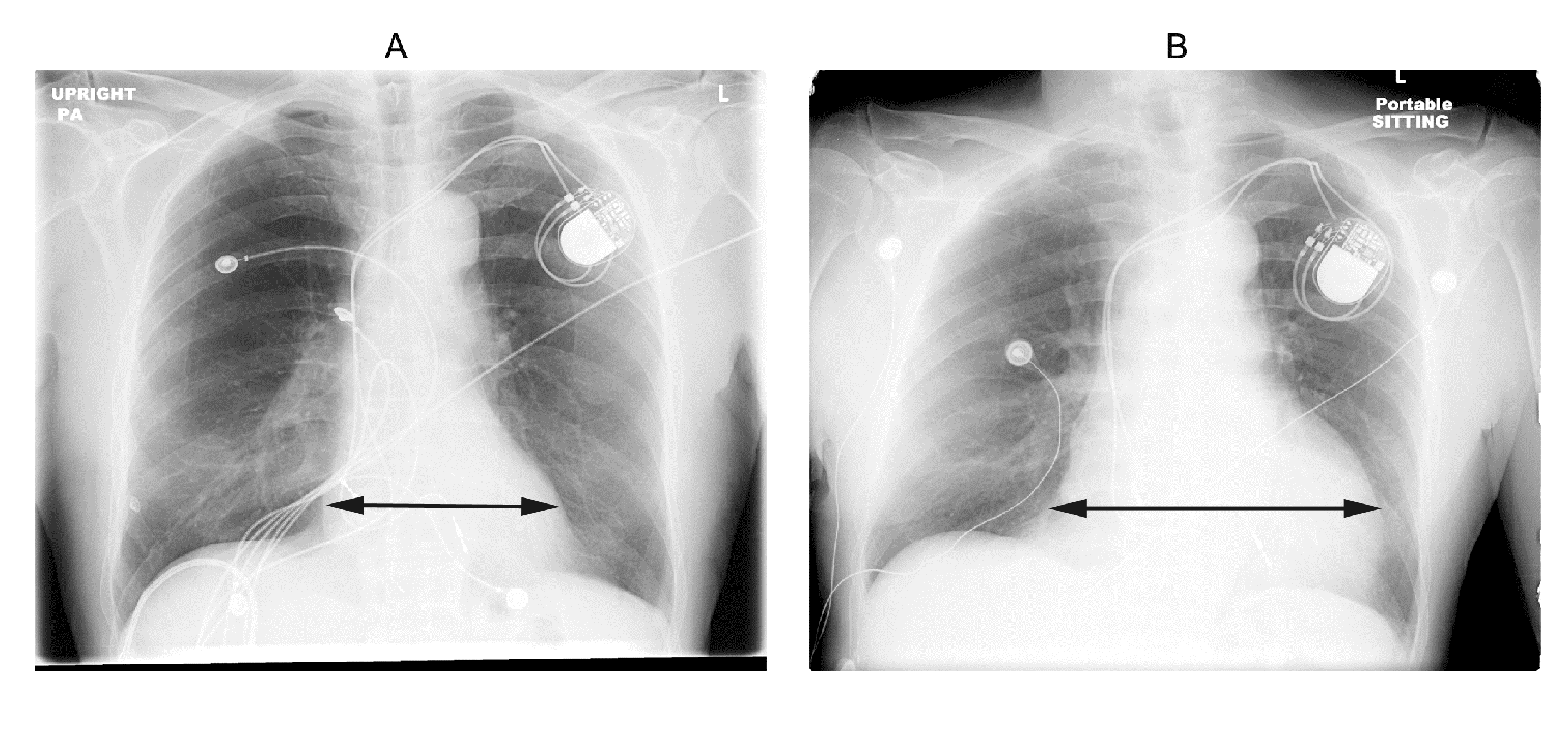
Chest Radiograph Appearance of Large Pericardial Effusion after Cardiac Perforation. (A) Immediately following the implantation of a pacemaker, the chest x-ray (CXR) shows a normal appearance of the cardiac silhouette. (B) At two weeks postoperative, the CXR (performed because the patient reported symptoms of chest pressure) shows an enlarged cardiac silhouette. The patient responded to pericardiocentesis with no lead repositioning. (Figure originally published by Williams and Stevenson 2012.)
Please check back with the Heart Rhythm Center for future podcasts:
Postoperative Care after an EP Study (and possible ablation)
Esophageal Proximity can be monitored to guide locations of ablation to help minimize risk of esophageal damage. The entire length of esophagus that is contiguous with the left atrial posterior wall can be visualized with intra left atrial ICE to monitor ablation delivery and power titration. [1] Figure 1A shows the typical location of the esophagus during an atrial fibrillation ablation. Ablation over the esophagus is avoided or power is titrated to minimize risk of esophageal damage. Endocardial thrombi or coagulum can be detected using radial ICE as shown in Figure 1B. Left atrial damage can also be monitored using radial ICE. Figure 1C shows an unusual case of a tear or rent in the endocardium discovered during an atrial fibrillation ablation. Finally, though radial ICE is not the ideal imaging modality to evaluate for pericardial effusions given its limited far-field resolution. Figure 1D shows the pericardial space in view when an intra-left ventricular ICE position is utilized.
Radial ICE to Monitor for Intraprocedural Complications.
Figure 1 Radial ICE to Monitor for Intraprocedural Complications. Image A shows the left pulmonary vestibule with catheter evident at 9 o’clock and the esophagus viewed obliquely at ~7 o’clock. Image B shows a coagulum versus thrombus adherent to the endocardium. Image C shows a left atrial endocardial tear that did not result in pericardial effusion. Image D shows the pericardial space when ICE catheter positioned across the mitral annulus in the LV.
References:
1 Ren JF, Lin D, Marchlinski FE, Callans DJ, Patel V. Esophageal imaging and strategies for avoiding injury during left atrial ablation for atrial fibrillation. Heart Rhythm. 2006;3: 1156-1161.